
This is the first in a series of three case studies illustrating success stories in preventing falls and injuries from falls. The series is brought to you by Posey. Watch for the next case study in the September issue of American Nurse Today.
Successful fall prevention programs use multimodal interventions, such as detailed fall risk assessments, frequent monitoring by staff, and appropriate use of equipment. Healthcare facilities typically implement best practices in bundles, making it often difficult to determine which interventions are the most effective.
UPMC St. Margaret Hospital in Pittsburgh, Pennsylvania joined the Pennsylvania Hospital Engagement Network (PA HEN) in April 2012 to reduce falls with injury. This set us on a path that resulted in a 75% reduction in falls with serious injuries. (See Falls with serious injury graph)
{kind=link}
Here is how we accomplished this reduction.
Analysis: Role of data and best practices
After joining PA HEN, we formed a multidisciplinary team tasked with reviewing and investigating all fall events, extracting and analyzing data, and evaluating best practices implemented as a result of root cause analysis.
The multidisciplinary fall team implemented prevalence rounding and post fall debriefing. Despite best practice implementation, we discovered variations and inconsistencies in our practice environment. We found that making sense of the data collected through a revised post-fall debriefing and delivering the information to staff in an easily understood format was the “magic bullet” in our success story.
Strategy: Debriefing
Debriefing engages staff, patients, and families while providing educational opportunities. Our debriefing process was critical for abstracting usable data. The facilitator who is responsible for debriefing the fall event needs to have expertise in the debriefing process to ensure data integrity. He or she must be objective and promote a nonjudgmental atmosphere of inquiry. The goal is to engage all participants, including the patient and family. At the end of the debriefing, the facilitator determines root causes and shares them with team members. Identifying root causes is invaluable to the debriefing process.
Root causes are then converted into frequency charts, which are useful for analysis and clearly illustrate the variables with the greatest impact on particular outcomes. Our team focused on tangible root causes, such as safety equipment, which proved successful in reducing falls in our facility. (See Case study.)
{kind=link}
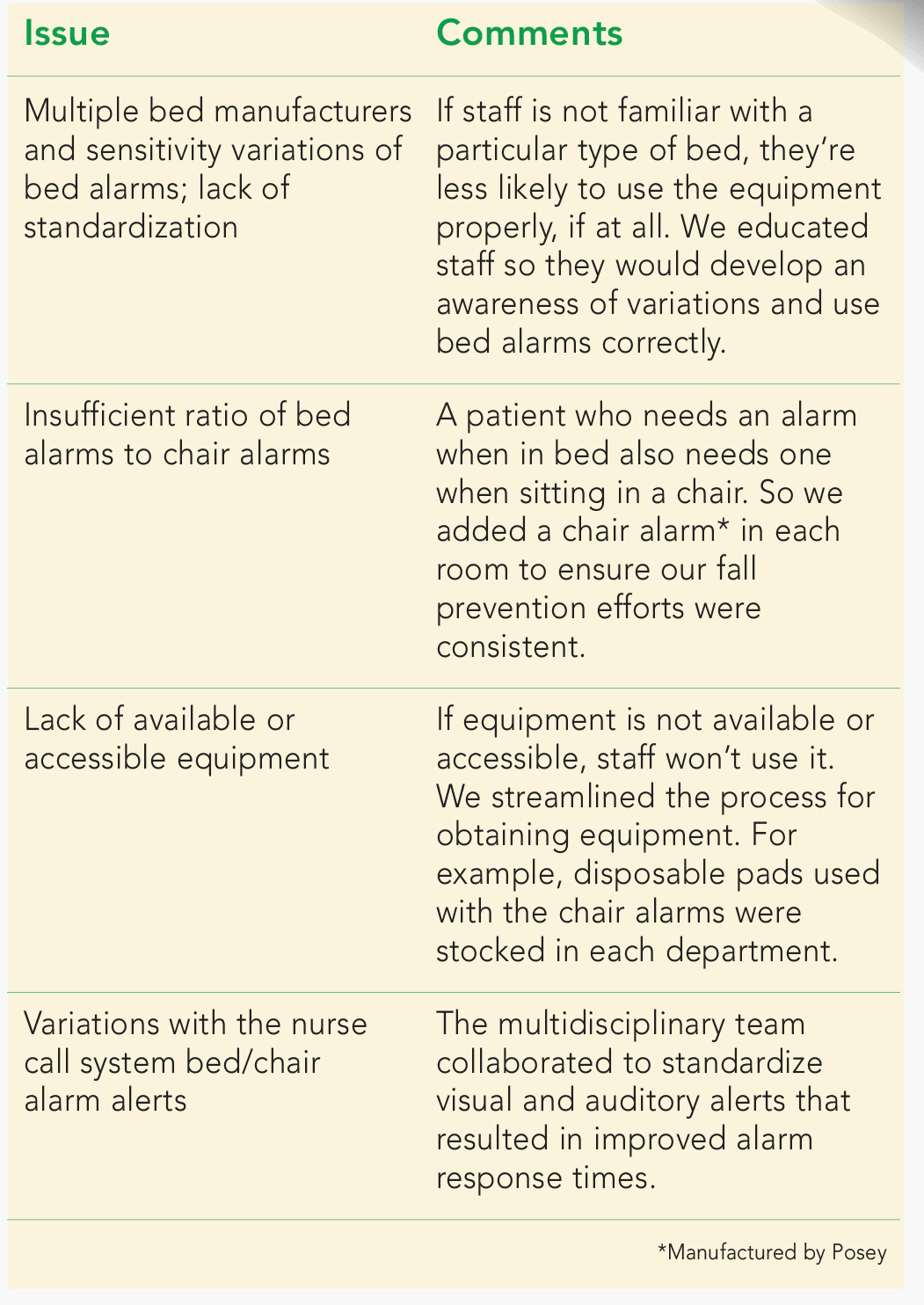
Strategy: Enhancing equipment use
Commonly used fall prevention equipment includes bed alarms, chair alarms, low beds, floor mats, and nurse call system/alarm integration. Based on its analysis of various types of falls and process-improvement initiatives, the team put interventions in place that essentially resolved identified equipment issues.
The debriefing process identified the following equipment issues.
{kind=link}
Outcomes: Falls reduction
In the first year of our initiative, we had a 50% reduction in falls with injuries and won the 2013 Hospital Association of Pennsylvania Achievement Award for Patient Safety.
We’ve achieved the following reductions over the past 4 years:
• 75% reduction in falls that resulted in serious injuries
• 60% reduction in falls that resulted in injuries
• 25% reduction in all falls.
Our ability to sustain these improvements keeps patients safer during hospitalization.
Kathleen Fowler, MSN, RN, CMSRN Quality Improvement Manager UPMC St. Margaret, Pittsburgh, Pennsylvania As told to Janet Boivin, BSN, RN