
Editor’s note: This is the second of three case studies describing success stories in preventing falls and injuries from falls. The series is brought to you by TIDI. Watch for the next case study in the November issue of American Nurse Today.
When hospital patients fall and suffer an injury, family members perceive that nurses and other hospital staff aren’t paying enough attention to their loved one. The Centers for Medicare & Medicaid Services (CMS) agree, deeming falls preventable events that should never happen in healthcare facilities. Consequently, falls with associated injuries can lower a hospital’s reimbursements.
Community Medical Center (CMC) is a 500-bed hospital predominantly serving the senior community in Toms River, New Jersey. In this population, the average age of Medicare beneficiaries is 72. Below we describe how we reduced the fall rate at CMC.
Analysis: TST participation
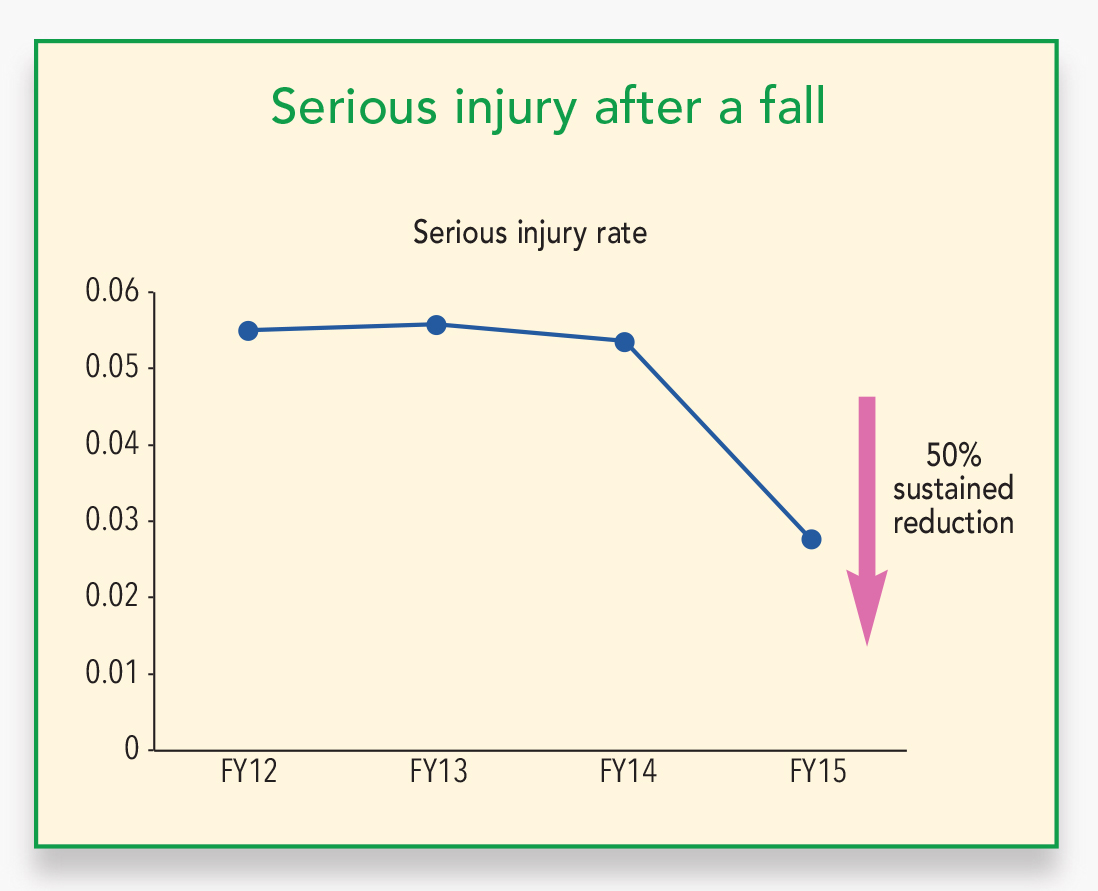
Our analysis showed that at CMC, falls are concentrated in the elderly patient population. To reduce the falls incidence, we participated as one of the pilot sites for The Joint Commission Center for Transforming Healthcare’s (CTH) project called Preventing Falls Targeted Solutions Tool (TST®). CTH describes TST as “an online resource that provides a step-by-step process to assist hospitals in measuring fall and fall with injury rates, identifying and measuring barriers to fall prevention, and implementing the Center’s proven solutions for falls prevention that are customized to address specific barriers.” Since the project launched in 2013, partner hospitals have shown a 35% reduction in patient falls and a 50% decrease in injuries caused by falls. (See Serious injury after a fall.)
{kind=link}
Strategy: Use an interdisciplinary team
CMC’s interdisciplinary TST committee used targeted solutions tools for falls on three units. The team included staff nurses, rapid response nurses, patient care directors, a risk manager, a chief nursing officer, an administrative director, an educator, a pharmacist, environmental services staff, clinical information system staff, and a facility operations manager. The three units were:
• Neurotelemetry: This 27-bed unit is a designated inpatient stroke unit and a level 3 epilepsy center. Patients here are considered at high risk for falls due to seizure disorders, movement disorders, functional deficits, cognitive impairment, and psychomotor deficits, including symptoms of alcohol and drug withdrawal.
• Wound care: Many of the patients in this 32-bed unit are on multiple medications and tethered to such objects as sequential compression devices and negative- pressure wound therapy devices.
• Telemetry: In this 31-bed unit, many patients are on multiple medications and tethered to SCDs, heart monitors, cardiac drips, or chest tubes. As in the wound care unit, many also are cognitively impaired. The unit’s layout makes it difficult to visualize patients who have an increased fall risk.
Strategy: Targeted solutions
One of the targeted solution tools CMC uses to reduce falls is a family sharing brochure on patient safety that includes a patient/family/nurse contract. The brochure explains the factors that make patients susceptible to falls when hospitalized, such as certain medications or neurologic conditions. On admission, the patient and family are asked to read and sign the contract, which emphasizes patient risks. (Click to view The contract.) Both the brochure and contract are printed on yellow paper, which is CMC’s color for indicating the patient is at risk for falls. By signing the contract, the patient agrees not to get out of a bed or chair alone; the family agrees that when visiting, they will ensure the patient doesn’t ambulate alone.
We also use hourly patient rounding by designated healthcare team members. This helps ensure that patients aren’t going to the bathroom alone because of long waits for assistance. During rounds, staff also help patients with repositioning and ask if they are in pain or need help reaching personal items not within arm’s length.
Outcome: Falls reduction
At the beginning of the TST project, we were required to input our patient database and information about past falls and injuries into a CTH site. We continue to monitor falls on inpatient units. Once a month we have a conference call with other project members to share ideas, initiatives, best practices, and outcomes. (Note: Patients who fall while off the unit, such as when they are in the X-ray or magnetic resonance imaging areas, are excluded from the program.)
Since joining TST, two units have consistently trended downward in falls incidence. Special floor mats are being used hospital-wide. We believe our reduction in falls results from the floor mats* and other prevention tools, such as color coding, family brochure, hourly rounding, and contract, which in turn have heightened awareness and vigilance about fall prevention. (See Case study.)
{kind=link}
The Preventing Falls TST is complimentary to Joint Commission-accredited organizations. It can be accessed through the Center’s website or the secure Joint Commission Connect extranet.
By Marley A. Nicolas, MSN, RN, Administrative Director of Patient Care Services; Cecile Gayanilo, MSN, RNC, Director of Neurotelemetry; and Kristin Bellas, BSN, RN, ONC, Director of Orthopedics and Joint Program Coordinator at Community Medical Center in Toms River, New Jersey As told to Janet Boivin, BSN, RN
Editor’s note: This is the second of three case studies describing success stories in preventing falls and injuries from falls. The series is brought to you by TIDI. Watch for the next case study in the November issue of American Nurse Today.